
- Title
-
Cellular and molecular mechanisms of repair in acute and chronic wound healing
- Authors
- Martin, P., Nunan, R.
- Source
- Full text @ Br. J. Dermatol.
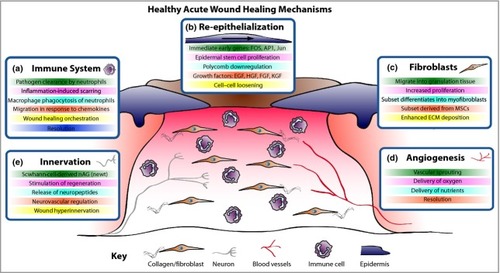
Acute wound healing mechanisms. The healing of an acute wound involves coordinated cellular and molecular responses. (a) Initially immune cells migrate to the wound site and, in addition to clearing invading pathogens, in part they also orchestrate the healing process. (b) Cut epidermal edges upregulate wound-associated genes, thus enabling collective cell migration. (c) Local and blood-borne fibroblasts proliferate and migrate to form the wound granulation tissue, provide structure and signalling cues and deposit new extracellular matrix (ECM). Some fibroblasts differentiate into myofibroblasts to aid wound contraction. (d) The wound bed is perfused with oxygen and nutrients through new blood vessels derived by angiogenesis. (e) Wound healing rates exhibit a positive correlation with innervation, but hyperinnervation after wound closure could contribute to neuropathic pain. EGF, epidermal growth factor; HGF, hepatocyte growth factor; FGF, fibroblast growth factor; KGF, keratinocyte growth factor; MSC, mesenchymal stem cell; nAG, newt anterior gradient protein. |
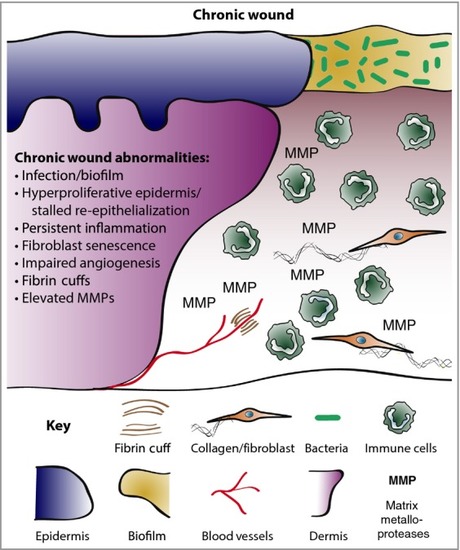
Chronic wound biology. Chronic wounds are often infected and exhibit a persistent aberrant inflammatory profile. Re-epithelialization stalls but wound keratinocytes are hyperproliferative. Granulation tissue is defective and does not nurture healing, in part due to elevated matrix metalloproteases (MMPs) and poor fibroblast infiltration. Neoangiogenesis is poor and fibrin cuffs restrict existing vessels, limiting the diffusion of oxygen through the wound, rendering the wound hypoxic. |
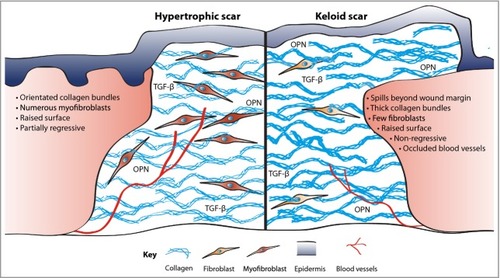
Excessive fibrosis. Scars, formed in part as a consequence of inflammatory signals, are comprised of collagen deposited in thick orientated bundles rather than the basket-weave-like fibrils found in normal dermis. Hypertrophic scars have excessive collagen deposition, leading to a raised surface that partially resolves over time. In contrast, keloid scars have thicker collagen bundles, extend beyond the original wound margin and rarely regress. Contractile myofibroblasts are prevalent in hypertrophic scarring but all but are absent in keloid tissue. Keloids can also be characterized by occluded blood vessels. OPN, osteopontin; TGF-β, transforming growth factor-β. |